This pamphlet is the second TRT instructional aid for the chemically dependent person. It explains how to do TRT Phase Two (The Matrix).
This material is for TRT participants. It also provides family members and friends information about the TRT program so that their support for the participant may be enhanced. The TRT Educational Program, including this material, is not intended for general interest reading. It is not a solicitation to engage in TRT. Neither is it authorization to provide TRT to anyone. TRT is authorized for use only under the supervision and facilitation of a Certified TRT Counselor. The authors of TRT, and or their designates, are the TRT certifying authority.
© 1988 Collins & Carson
Welcome To TRT Phase Two
TRT Phase Two is also called the Matrix because its form (fig. 1) consists of five interrelated columns that, when utilized properly, detail on one page the many effects each experience of trauma has had on the person. The form also is intended to paint a broader picture of the effects of the experiences of trauma as a whole. Through the detail and the particular way in which the experiences are framed, most victims of trauma find loss much easier to identify and reconcile.
Fig.1
The Matrix (TRT Phase 2)
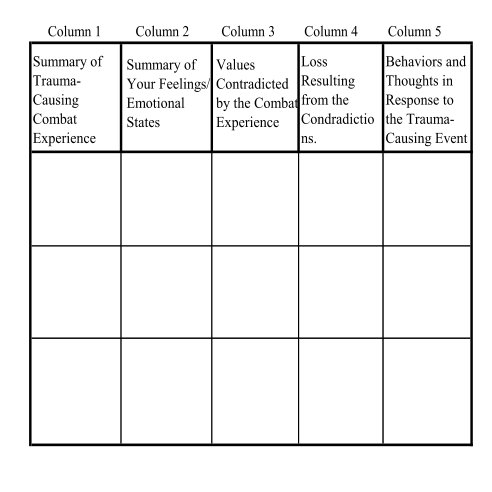
The Matrix is completed by applying each of the trauma-causing experiences descibed in Phase One across the five-column form. The Matrix should be filled-in one incident at a time beginning with the earliest incidents of chemical use influence. Except for a few sample applications of the Matrix, all the trauma-causing chemical use experiences should be recorded onto the Matrix’s form before you share your writing with your group.
Writing
Column 1 provides the transition from Phase One to Phase Two. The column’s purpose, then, is to facilitate your change in focus from the events themselves to the effects those experiences had on you. Consequently, the emphasis in Phase One is lessened as you describe the incident in summary fOIm only. For example, a long description of a drinking episode in which aberrant behavior and the experience of being arrested (along with the overwhelming toxicity) were the principal trauma-causing event, would be recorded in column 1 simply as “arrested.” A brief record of the behavior precipitating the arrest might also help to summarize the incident accurately. This is especially true if multiple incidents involved similar experiences of trauma; for example, recurring episodes of driving while intoxicated DWl or DUI) or arrest for assault. Under such conditions, column 1 would appear as follows:
Remember, the intent of TRT is not to teach you to remember how “wrong” or “bad” you were so that you will work harder at staying sober or being more responsible, or in any other way at being a better citizen (See Choice. Grief, Trauma and Control: An Explanation of Why and How TRT was Developed). Rather, the recording of these experiences in this summary fashion is to help you remember the different losses resulting from the several events as separate and specific experiences so that they may be addressed individually and, eventually reconciled completely. The next three columns address that very important endeavor.
Column 2 summarizes the emotional experience associated with each aberrant chemical-use episode. You should expect the toxicity during the incident to hamper substantially your recollection of your feelings at the time. However, sometimes, strong feeling states will emerge when you are given the opportunity to remember. In addition, as in the first phase, what you feel today in response to that past episode will suffice.
When summarizing feelings, be sure to separate those recollections that reflect shock. This particular state is hallmarked by disbelief, numbness, the feeling of being separate from one’s. self and dissociation. It is very important that you have the opportunity of recognizing those experiences as the entry into shock that accompanies trauma and as an indicator of at least temporary incapacitation.
Column 3 addresses those values that were contradicted by the chemical-use behaviors. Such values are usually those things in which we believed deeply ourselves as well as those values handed down to us in our relationships with other people. Either way, values are usually being represented in our language when we speak in terms of what “should” be or what is “supposed” to be. In this column, then, we ask that you state what values were contradicted by the chemical-use experience you have summarized in the first column. Once you have thought these things through, we ask that you record them in as abbreviated a way as possible in column 3. Use the first person (“I,” “me” or “my”) when referring to your beliefs. Once you have listed those values contradicted by that one drinking/drug use episode, move on to column 4.
Column 4 is the place where each loss resulting from the belief-contradicting traumatic experience is identified and so made available for reconciliation. This column is completed by looking back to the contradicted values and beliefs recorded in the previous column and concentrating on what you lost as a result of those contradictions (see Appendix). As the losses begin to make themselves known, write them in an abbreviated form in the space you made available in column 4 (Fig. 2).
Column 5 helps you focus on those thoughts and actions that were used to protect you from your experience of the trauma. As in each preceding step, you should pause and recall the event. In this recollection, your focus should be on what you thought and may have done following the experience. Sometimes, protective responses occur immediately. At other times, they are delayed as much as several days and even come in recurring patterns as they are needed. Examples of protective thought processes are denial, lying, elaborate schemes of cover up and radical cohersion of the environment (relationships) to comply with the protective perceptions and methods. Protective survival responses range from absolute repression and the view that “nothing happened” to the new belief that “I must have really wanted this to happen. Thus I am insane, very bad or evil.” An example of how to write protective responses into column 5 is available in Figure 2.
Fig. 2 Complete Description of An Episode in the Matrix

The example in Figure 2 is a traditional example of the Matrix’s use by people being adversely affected by their own chemical use behaviors. Sometimes, however, the drinking/drug use experience is traumatic in more complex ways. For example, many people, especially women, find that during the period in which toxicity interfered with their ability to control themselves, they became vulnerable to and consequently victims of externally generated intrusions, such as sexual assaults. Such intrusions coming at a time of high toxicity often result in compounded confusion. When applying such a trauma-causing incident to the Matrix, denote both experiences in the first column. Both will have precipitated emotion, contradicted values, and brought loss and protective responses. In addition, those combined effects are usually recalled together. In these specific cases, it makes no difference that the two victimization events are recorded together as if from a single experience (Fig. 3). The only requirement is that the incidents be described without the use of self-blame or any other depreciative method. Remember, the “should’s” and “supposed to’s” are used only as indicators of values and beliefs. Such words are meant only to help identify those beliefs and values, so that the subsequent loss may be ascertained and then reconciled. The “supposed to’s” and “should’s” are never meant to connote that some form of action is necessary through judgment or change in belief or behavior. Such a shift in thinking is usually the antithesis of what is needed to complete the grief experience successfully.
Fig 3
Recording of an Episode Causing Multiple Trauma

Reading
The Matrix is usually read differently from the way Phase One writing is shared. In that phase, the concentration was on identification that the event(s) occurred. Experiences residing in the subconscious as current incidents were being brought forward as they actually were, traumas that occurred long ago. The reading process was individualized to slow or accelerate itself, depending on the time required to tell about each newly recalled experience. The second phase is also individualized to the extent that each description is shared individually. However, other equally important processes are occurring. First, this time, the events that are being described have already been shared once. This stage offers, not only experiential understanding, but also a cognitive perspective on the effects the trauma has had. We have found that reading each incident as one did in the first phase actually slows the cognitive progression and reduces the total benefit of the Matrix. Consequently, after several sample incidents have been shared for purposes of getting the form correct, the Matrix is usually read a number of incidents at a time and without as much individual processing between incidents as occurs in Phase One. This approach should help you to achieve a balance between processing the experiences in terms of their individual effects and processing them collectively in terms of their combined effect as one life event. Your TRT counselor will help you to determine how to read your Matrix in a way that is appropriate for you.
Appendix A:
Levels of Loss
Losses go to the core of an individual’s psyche at three basic levels. First, esteem and its loss involve what we call the individual or intrapsychic level. This level is concerned principally with a person’s ability to know himself or herself. Losses here are strictly personal. Second, trust and respect and the loss thereof are features that underpin the person’s interactive abilities. Such abilities are necessary for us to have intimate and real relationships. Thus, we call the results of interactive-oriented intrusions relationship losses. Third, losses of a role model and of family esteem occur at an even deeper level than the one-to-one issues reflected by relationship losses. Intrusions and subsequent reductions in capacity at these deeper levels impair that aspect of ourselves that functions in groups, organizations or any system in which multiple relationships are overlapping individual ones. We call these particular experiences systemic losses.
Identifying losses into these three levels may be helpful at this stage of TRT, but what we must keep in mind is that right now, the most important consideration is that the loss Occurred. Its meaning to us is not as important at this time. In other words, we want to concentrate on feeling the losses that are being identified and not risk interrupting the emotional passage by intellectualizing (thinking) too much. Consequently, we ask that when you list losses in the fourth column of the Matrix, that you do so without identifying the loss’s personal, relationship or systemic features.
Later, when TRT is being completed, we will combine these losses with others that will be discovered and, at least in part, reconciled through TRT’s Phase Four. At that time, all the losses reflected in both Phases Two and Four will be combined onto one form. Representing the losses together and in order according to their various levels usually provides even more understanding and meaning to their occurrence than is usually experienced by most participants at this second stage of the loss resolution process.
The next pamphlet explains how to do the third and fourth TRT Phases for chemically dependent people. The pamphlet number is: I-Ee