This booklet provides an overview of the basic theory underpinning TRT. Although the material is written for the layman, it contains some technically oriented information. It is presented with the intent that the material will be read in conjunction with the TRT participant’s passage through the trauma resolution process. The booklet’s number is:
V-C
Personal Reality
We begin with a focus on a fairly traditional view of how we are constructed psychologically. An analogy often used to exemplify how our personal reality systems are formed is that of a complex weave of threads that eventually becomes a finished suit of clothes. Values, beliefs and individual image link into psychological thought and being. These thoughts become the “threads” of the various components of the materials. One entire section or layer of the cloth may represent a developmental cycle such as during the period of adolescence or entry into the adult life of parenting. Another part of the weave may be the values and beliefs that comprise the relationship to a spouse. A separate layer of cloth may be the interrelationship of thoughts which provide the belief system through which a person intellectually conceptualizes God or relates to the nation. As value and belief are interwoven, they come to comprise the psychological reality of the human being. This aspect of ourselves has been called the “the warp and woof” of who it is that we are.
Fig. 1 Values and beliefs are the same to the system of reality that threads are to material.
Values and Beliefs
When intrusion occurs, values usually are contradicted and, in our model, threads are torn apart. For example, most individuals believe that people should endeavor to co-exist without becoming aggressive or violent with others. Consequently, when victims of crime or those involved with chemically dependent people are exposed to such aggressive or violent actions, beliefs are contradicted. Similarly, military or law enforcement personnel, although trained in methods of waging war or in other ways aggressively countering violence, usually believe, personally, that people should not hurt each other. Consequently, their exposure to destructive and threatening behaviors contradicts those values of how people are supposed to behave.
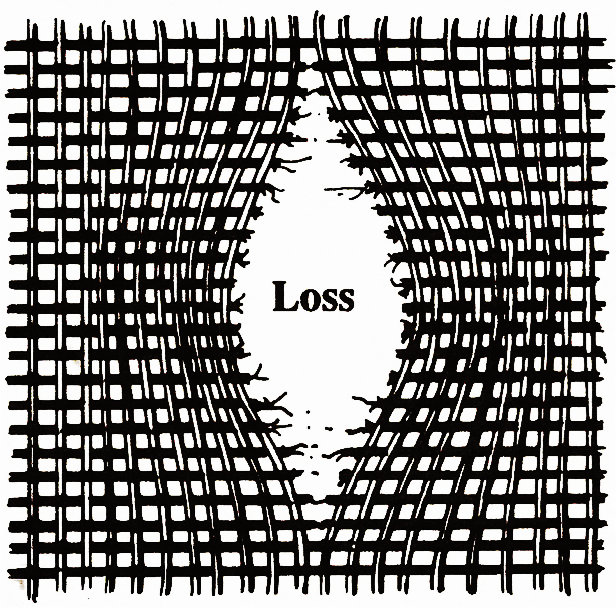
As these values are contradicted or, worse, impacted so violently that they seem shattered, the weave of values that comprise the fabric begins to unravel. As a thread of thought undergoes the equivalent of being broken, that single thread becomes the start of a gap within the cloth. Additional assaulted values result in greater damage to the layers of material. When intrusion becomes violent, the fabric is ripped apart, separating the once-whole personality from parts of itself. The gap that results from the breaking of one thread or the tearing of the entire fabric is the void and vacancy of loss (Fig. 2).
Fig. 2 Torn threads (contradicted values) produce a void -loss
As we move into the damaged area for a closer view, the relationship of loss to emotion becomes more clear. We know that loss is almost always accompanied by shock, denial, anger, depression, guilt and sadness. We also know that when these emotions are a response to loss, they are usually experienced in that same order. Consequently, for purposes of graphically representing the complete loss experience, we conceptualize the process and its attendant emotional responses as a chain (Fig. 3).
Fig. 3 The loss process and its emotional responses are conceptualized as a chain.
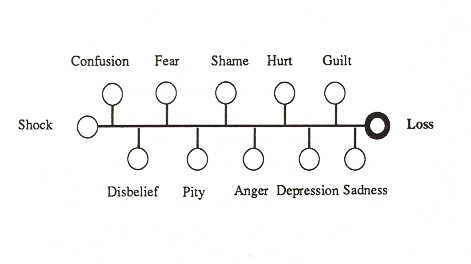
At the end of the chain is the loss itself. Connected to the loss are the emotional responses to it with the most protective states; i.e., shock, confusion and disbelief, at the end of the chain and furthest from the loss. In between are the more forceful emotions of fear, shame, anger, and depression that are usually experienced in the middle phase of the loss resolution process. Nearest the loss are hurt, guilt and sadness, which direct the final quiet passage through our vulnerability to the identification, acceptance and reconciliation of the loss itself.
In general, if all of these emotions could be identified, experienced, expressed and passed through as they appear consciously to us, then the problem (the loss) could be identified, accepted, understood and subsequently reintegrated into the person’s reality system. However, when trauma occurs (especially when it occurs frequently), the relationship of loss to emotion becomes more complex. As additional threads are broken, the gap widens: more losses and their accompanying emotional responses. In our conceptualization, each new loss chain is formed close to the others. As loss upon loss fades from awareness into the subconscious, the losses, each with its attendant emotional chain, become linked (Fig. 4).
Fig. 4 Loss Chains align parallel to each other.
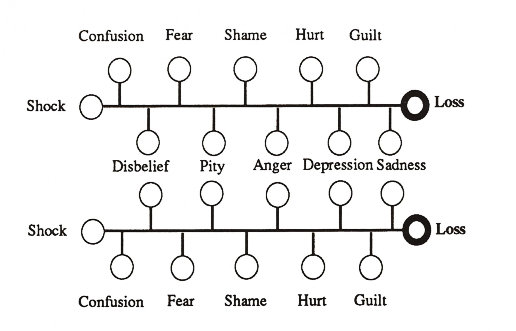
From this perspective, as the chains align parallel to one another, the similar emotions associate as well. For example, disbelief: confusion and shock are located at same ends of the chains, while in the middle pity, shame, anger and depression find their counterparts and come together as well. Finally, hurt, guilt and sadness position themselves to connect with their counterparts at the end, completing the combining process.
Of special importance to the loss/emotion relationship is the description of how particular losses are retained in memory based on their origin. Where losses result from similar sources, they are clustered because of the relatedness of the values and beliefs being intruded upon. For example, a child assaulted by a violent alcoholic has lost self-worth, self-esteem, trust and respect because her values relating to her relationship with her father have been contradicted by physical assault. As these losses become a part of the subconscious, they are linked by a common bond. The commonalities are the multiple contradictions to the child’s beliefs that a father is not supposed to behave violently. The spouse of a chemically dependent person loses security and belief in the prospects for a continuing marriage. These losses combine with the many others resulting from the perceived origins of aberrant drinking behavior. Parents’ losses of family pride, role model and caring relationships resulting from the addiction’s control of their child combine because they are all viewed as coming from the drug-induced behaviors. And chemically dependent people themselves begin to cluster those losses of self-esteem, self-worth and self-respect that result from the drugs’ effects on their own lives. Military combat personnel cluster their losses of security, of a belief in a continued existence and sometimes even of the meaning of life in response to the values contradicted by the death and destruction of war. People who work with abused and abusing people cluster losses of trust and respect as well as losses of the view that people are humane or “good.”[1] The alignment and cluster process is reflected in Figure 5.
Fig. 5 Losses, resulting from the same source of trauma, cluster.

1Mental health or crisis management professionals adopt necessarily tough (self-protective) approaches to the process of helping others. However, those individuals’ personal values are still effected by the helpers’ experiences of the victim’s trauma (see the TRT series for Crisis Managers)
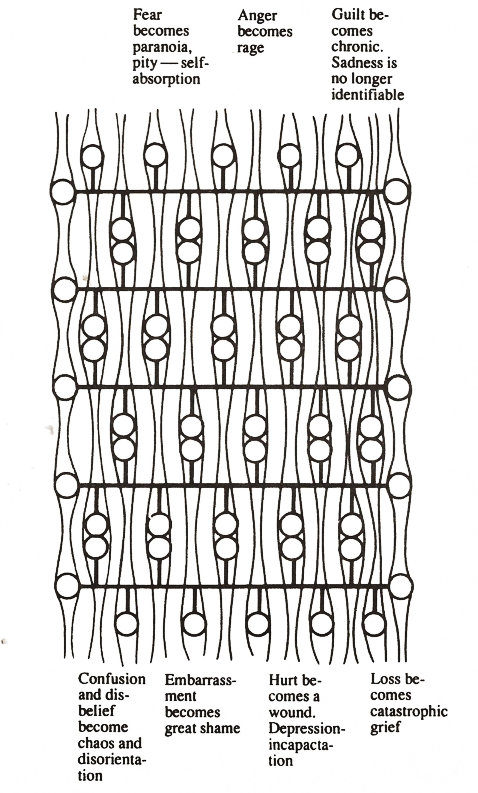
In addition to the clustering effect’s influence, we view trauma as perpetuating itself through another phenomenon. The re-exposure to the ever-present attack on values forces the loss chains together, much as threads fused together by heat. As the pressure is increased, the stress is compounded. Eventually, the various emotions in the once-separate loss chains form connections with their counterparts close to them. The more fused the loss chains become, the more readily the individual emotions comprising the chains connect. As the cluster of losses grows, the connections become so pronounced that they form streams of same emotions that flow across the individual fibers of what was once separate loss processes (Fig. 6).
Thereafter, when an individual experiences one of these emotions, such as anger, the many angers tied together in the memory evoke a disproportionate reaction: rage. To take other examples, embarrassment becomes great shame and grief catastrophic grief. In addition, development of the streams phenomenon produces something quite different from the original singular repressed loss experiences. This new conglomeration of emotional currents and unreconciled loss chains is a single formation that fuels the ever-continuing survival/victimization processes.
Fig. 6 Parallel loss chains form connections of like emotions. The connections eventually become like streams of emotion flowing across the once separate loss processes.
If we could observe the newly generated loss formation physically, it would begin as a tiny hole in the vast fabric of the psyche. As continuing destructive events unfold, the tear in the fabric of personality would become deeper and wider. As the loss becomes more formidable, the rest of the psyche responds by offering healing mechanisms just as the physical body supplies white corpuscles to combat an infection. Such offerings include subconscious adjustments in thought and perspective that attempt to ameliorate the damage. For example, people believe they can withstand the infraction, and they trust that with time the Rain will be lessened as the wound heals naturally. Where losses are singular or not so intense and not clustering from similar causes, the natural grieving process works, often subconsciously, to process the inherent shock, denial, anger, depression, acceptance and understanding stages.
The Maze
For persons experiencing multiple or very intense trauma, however, the continuing impact and constant failing of the mind to reconcile loss fuses and hardens the new formation into what we call a Maze of emotional circuitry. The result is the blurring of the individual identities of the loss chains. Consequently, the otherwise natural human healing processes cannot provide the necessary solutions.
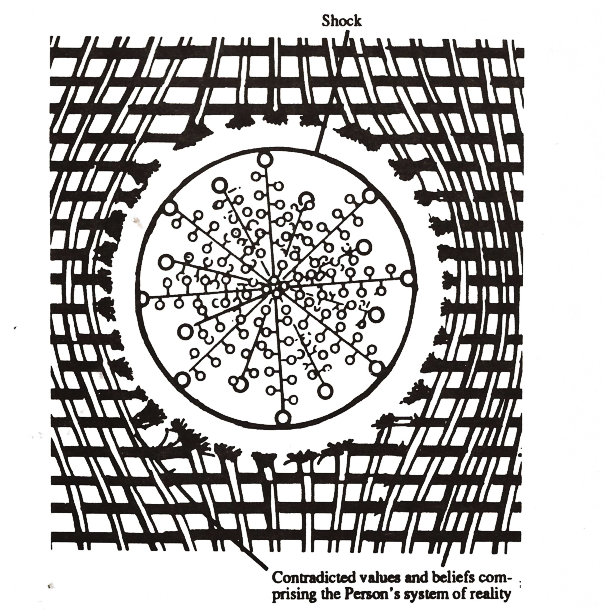
As the Maze grows, it soon begins to protect its own existence. Foremost among these protection mechanisms is the experience of shock. In a linear diagram of the Maze, shock is represented as existing at the outer end of the chain of emotions. However, in a multi-dimensional view of the Maze, shock wraps itself around the entire formation of emotional pain and loss. The combined physiological and psychological reality of the shock then acts as a protective shell or coating entrusted with the task of preventing the person from knowing the true extent of the damage inside (Fig. 7).
Another fundamental protection mechanism available to the Maze is unit synergism. A system or unit (such as this network of loss and emotion) is made up of integrated parts that function for the benefit of the whole. As these parts become more interrelated, their identity is given over to the power of the whole. “Synergism” is the expression that describes this wider power or unit force. Synergism implies that unit force has a power greater than the sum of the unit’s parts. For example, a team composed of nine players would have a unit synergism representing the team as the tenth component.
Fig. 7 Shock acts as a protective shell or coating that prevents the Person from knowing the true extent of the damage inside.
The problem in understanding synergism is that it is never represented by a physical entity but by the less-clear interconnectedness of the system’s many parts. Consequently, synergism is an abstract force that is often clearly evident for those outside the system and usually only felt intuitively by those comprising its structure.
The primary responsibility of synergism is to protect and maintain its system’s existence. As shock surrounds the emotional pain and loss resulting from the clustered experience of trauma, the formation automatically produces a synergistic response that reproduces its own strength for the purpose of meeting its perceived responsibilities of providing protection.
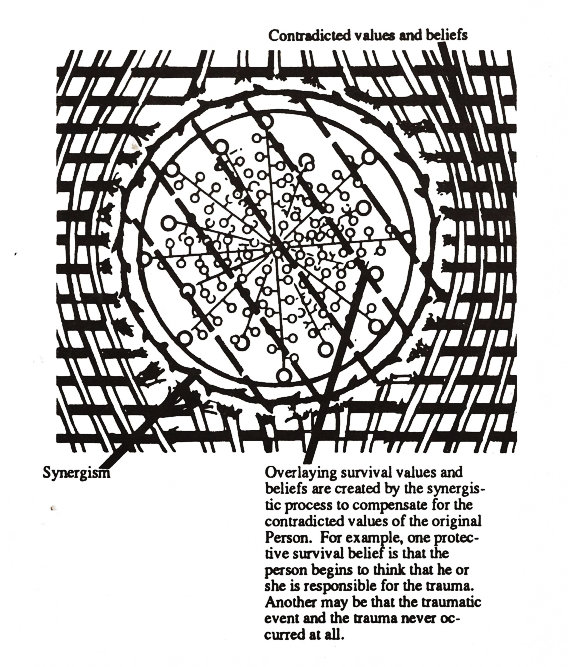
The synergistic effort accomplishes its protective task by filling in for or supplanting the wider reality system’s reduced capacity (trauma induced) to right itself. At the heart of the incapacitation is the physical reality of different brain functions. The original threads of the material torn apart were spun from the very fibers of personality that are responsible for solving (or “righting”) our problems. These are the very powerful abstract thinking, rational and cognitive aspects of ourselves through which values and beliefs are given form. Consequently, when those important threads are separated or damaged, they can no longer rely upon themselves. Asking those fibers to solve the problem of the loss of a part of themselves is, in actuality, asking the impossible. Consequently, the newly formed protective synergistic process compensates for that system’s deteriorated condition and begins to provide through the survival process, a new set of beliefs, values and problem-solving mechanisms (Fig. 8).
Fig. 8 During the survival process, synergism creates new beliefs that cover over the trauma.
As the Maze of losses grows, the synergism protecting the formation’s existence eventually becomes an active apparatus that can lobby very aggressively with the rest of the psyche for the new loss formation’s predominant right to the available psychic focus. All abstract thought and associated behavior that emerges from the synergism’s influence on the psyche during the Maze’s growth is created for the dual purposes of ensuring that (1) the Maze of losses is not recognized by the rest of that psyche and (2) the Maze remains intact and undisturbed. If the trauma goes unresolved for a long time, the synergism’s protective interactions with the rest of the psyche will eventually be negotiating for total control of the person. In this way, unresolved trauma becomes its own self-perpetuating life force, distinctly different (separate) from that system of values and beliefs originally thought of as the Person.
Because the crux of the Maze is incompletion, failed resolution, and emotional pain, the Maze’s synergistic power, operating from its paradoxical position of both protecting the person as well as hurting him or her by keeping the trauma intact, often takes the form of incongruity, non-reconciliation and intensity. The protection mechanisms generated are usually dichotomy of thought and behaviors with conflicting purposes and outcomes. The individual suffering such a problem begins to believe on the one hand that his or her world is coming to an end and on the other that what is happening really isn’t that bad at all. This person’s behaviors will in part attempt to prevent the attacks or assaults from occurring and at the same time function as if that person were completely incapacitated and incapable of stopping the trauma-causing events. From this two-part approach to life arises the phenomenon of self-blame and an illusion of control that prevents even more resolutely any trauma reconciliation efforts.
The Second Maze
Where the initially experienced trauma is an extremely destructive process, the protection system that is extended past that initial period eventually produces more damage. As the survival system takes control, the survival responses themselves, functioning rationally to deny or avoid the internally retained trauma, function irrationally from the perspective of the old values. Beliefs in honesty, integrity, socialization, reality, caring, intimacy, trust, respect and how the person is supposed to function in his or her role in life are contradicted by the demanding survival responses of lying, withdrawal, isolation, illusion, unconstructive fantasy, narcissistic self-centeredness, and some forms of compulsive obsessive behavior[2]. The paradox of such responses – being natural and expected from the point of view of the internally retained trauma but not natural to the more congruent system of ordinary existence-divides the individual into further incapacitation. The result of this dilemma is the internalization of more loss.
2Many kinds of compulsive behavior are found to result from brain chemistry and are not necessarily related to trauma.
Like the loss resulting from the initial trauma- causing event(s), these losses cluster together. The common sources are the threads of values severed by the survival protective responses that contradict those values. For example, when a spouse of a chemically dependent person who, out of survival, covers up or lies for that person, this behavior contradicts values of honesty and straight-forwardness. New losses resulting from the contradictions are of self-esteem, self-worth, self-respect and self-trust. In addition, the individual loses intimacy, socialization and any real relationship with those to whom the cover up is directed. Out of the need to survive, battered spouses create the illusion that the beating is not occurring. Perpetrators of such abuse do the same thing. Contradictions are the essence of those persons’ senses of reality as the illusions are created by the protective response. Aside from the losses of self-esteem, self-worth, and self-trust, there is a loss of reality and of the ability to manage one’s own life. Vietnam veterans, law enforcement officers and child protective service workers functioning in delayed survival reactions lose intimacy, companionship, trust and the ability to receive and give caring as they otherwise normally would.
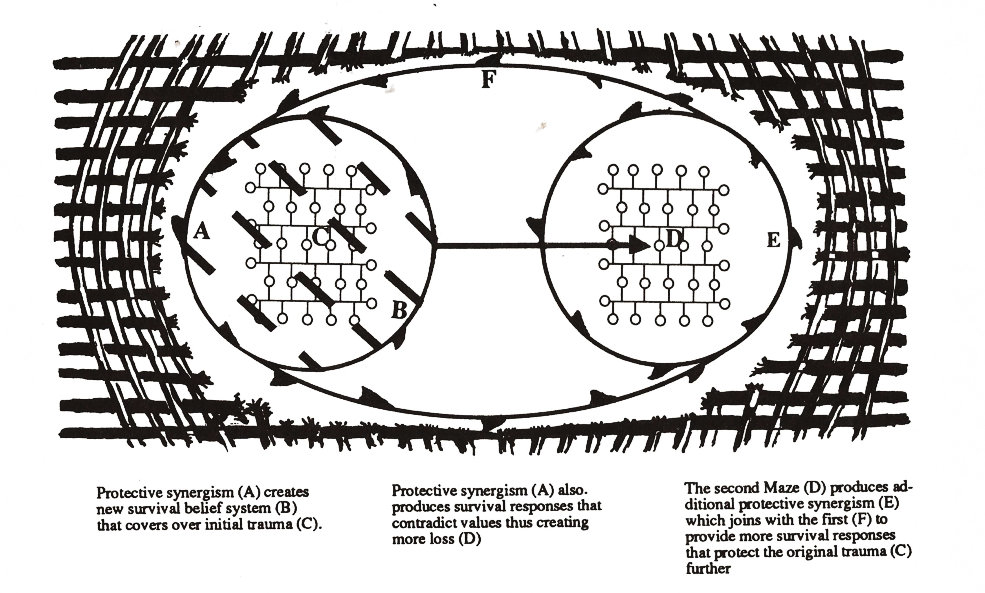
Again, the clustering of the different losses produces its own formation. Only this time, instead of the losses having only one source, they have two. The first is the person’s own survival behaviors that contradict the original person’s values. The second is the still-unresolved trauma and loss comprising the first formation or Maze that generates the fuel for the ever-needed but continually contradictory survival responses. Because of the two real causes of the second loss formation, this second Maze is joined to the first. Eventually, the synergisms stemming from the two separate clusters of loss combine to protect the entire experience of hurt as a single internal process. Figure (9) depicts the relationship of the two Mazes as the graphic portrayal of the total trauma and post-trauma experience.
Fig. 9 Trauma and its effects
A Dilemma
Herein lies the great dilemma for victims of trauma as it has continued throughout the ages. The original trauma has to be denied by the individual’s system of survival. The individual’s social system usually supports that protective endeavor by denying the trauma as well. For example, spouses of alcoholics have believed of themselves as well as having also been told by helpers for years that they (the spouse) either consciously or subconsciously planned to enter the destructive relationship in order to meet a pre-existing and sick need. In this way the spouse was helped to deny the trauma of the experience by accepting responsibility for having wanted and planned the outcome. The same diversionary acceptance (assignment) of responsibility approach has been applied to Vietnam veterans, law enforcement officers, rape victims, battered spouses and even people traumatized by genetically based diseases. Through this environment of individual and collective protection of the trauma, the original trauma itself, including the trauma-causing event, is seldom ever available consciously to the problem solving apparatuses. Rather, the only available indicators of dysfunction are the very visible survival responses.
Consequently, almost all problem-solving endeavors are oriented toward emphasizing the damage brought about by the survival protective responses. Incredibly, in such cases, the individual’s attempts to understand and resolve his or her situation are themselves so influenced by the survival process that such problem-solving efforts are being controlled from the onset by the original trauma.
In other words, when such an emphasis (i.e., seeing the survival responses as the “the problem”) is applied to the survival response, the survival system is actually reinforced. Specifically, the Survivor will do anything to deny that the original trauma has occurred because the pain of that trauma is the fuel or life force of the Survivor’s very existence. Consequently, as problem solving is initiated, the Survivor protects the original trauma by accepting responsibility for the Person’s condition. Such acceptance of responsibility gives the impression of introspection, solution and a return to control but in reality preserves the fuel for the Person’s dilemma. The manifestation of this experience is the trauma victims’ exclamations that they caused their own problems- i.e. they were attracted into alcoholic or physically abusive marriages because they came from an alcoholic or other disruptive home, they were raped because they had asked for it, they fought in wars because they were basically aggressive or they developed cancer because they had not attained adequate spiritual direction in their lives.
In fact, our work has led us to conclude that the answer to trauma resolution does not lie with the individual at all, because the paradoxical system of survival that has controlled the person since the trauma occurred cannot be overcome alone. Rather, the answer lies with another individual’s ability and willingness to provide the necessary care and assistance to the trauma victim so that the Person can fully grieve what has happened to him or her. Once the individual is given this simple assistance, the paradoxical control apparatus will be gone, self-blame and self-abuse through inappropriate assumptions of responsibility unnecessary, and the individual freed to utilize his or her ordinary system of personal management.
Resolving Trauma
Resolving trauma when the rational cognitive thought system (values and beliefs) in which the trauma occurred is impaired can indeed be difficult. Add to that difficulty, a determined stoic and self-blaming system of thought and behavior, and the task of resolution may seem impossible. However, the task need not be so hard if the secrets of successful resolution are understood and their principles followed. There are only three secrets. The first is that the Mazes of loss must be approached in a way that reduces the inherent power of the protection mechanisms.
The second is that while that approach is being made, the need for the protection mechanisms must be brought to an end. The third is that complete trauma resolution with TRT can only be achieved if the individual is not sedated (includes periodic social[3], medicinal or addictive psychoactive drug use) during the period commencing with the beginning of the therapeutic experience and continuing until it is finished.
The first task that of reducing the protection mechanisms’ awesome power, is accomplished through special TRT individual or group therapy processes. The person or people who comprise these helping processes have an important function: to lend themselves temporarily to the trauma victim by sharing that person’s grief (See Giving Feedback in TRT). When this occurs, the survival responses are not needed.
3In addition to the more obvious problems a toxic central nervous system can cause a therapy session, the trauma resolution process can also be adversely affected if sedatives (including alcohol) are used on days other than when TRT is actually conducted. For example, if a TRT session is held on a Wednesday, the therapy will initiate a specific aspect of grief resolution that will continue to be addressed at both conscious and unconscious levels throughout the week. Should the participant drink for social or entertainment purposes on a Friday or Saturday, the central nervous system will be temporarily anesthetized. Even though the anesthetic effects are only temporary, they will still block the otherwise naturally progressing grieving experience started on Wednesday. The net effect of the periodic use is that the survival / protective system of thought will be supported. This support is analogous to the springs of a trampoline that keep the canvas taut so that it always bounces back to its original position. In other words, a TRT participant can work very hard in the TRT session, and then unknowingly reverse his or her achievements through the temporary sedations.
At the same time that the influence of the survival responses is being lessened, the shock that has surrounded the Mazes of emotional pain and loss must be experientially processed. This means that the individual must pass through the experience of the shock related to each trauma-causing incident consciously identifying the process as he or she progresses through it. Immediately, the protection mechanisms, which have delayed through their stoic activities the grieving process’s completion, will cease their extension of that process. The person will then be able to progress through the rest of the grieving experience at a pace that is natural and appropriate for him or her.
The second task, that of ending the need for the survival/protective processes, requires that each loss in the original loss formation be specifically reconciled before anything else is done. General recognitions that the individual lost self-esteem as a result of abuse, disease or war is not enough. The reconciliation of specific losses tied to specific contradicted values and beliefs is the key to trauma resolution. For this to occur, the first Maze must be dismantled one loss chain at a time. This is accomplished by identifying each trauma causing incident and each resulting loss chain. The chain must then be separated from the others so that the individual emotions may be heard and the negative power resulting from their repression expended. Once this is completed in the order in which the emotions are reflected in the chain, the loss at the end of each chain will become consciously available to be identified, understood, and integrated into today’s reality. Simultaneously, the broken threads of value and belief will be reconnected where appropriate or possible, permitting the damaged area of the fabric to be rewoven until the part of the cloth damaged by the original trauma-causing event is mended. To help the trauma victim accomplish these objectives is the function of the first and second phases of TRT.
Only after the first formation has been completely reconciled can the survival responses and subsequent losses be addressed. In addition, the cardinal rule of trauma resolution is to do nothing that makes the survival responses feel even more responsible in their protective efforts. Consequently, the second formation must be reconciled like the first, but with the additional stipulation that no effort be made to change the survival responses during the resolution process. Any such effort will only strengthen the survival responses’ attempts to maintain .their existence through subversion of the resolution of the last remaining experiences of loss. If the survival responses are not emphasized, they will, in most cases, automatically become non-existent as the remaining losses resulting from the tragic experience are grieved. Simultaneously, the threads of value tom apart by the changing survival responses will be rewoven and the Person thus regained. To assist the individual in accomplishing this objective is the purpose of the third and fourth phases of TRT.
The last phase of TRT helps the person to summarize who he or she was prior to the trauma, the trauma resolution process itself, and who he or she is now that the trauma has been resolved. This look back helps to finalize the trauma and the trauma resolution experience.
In the last outcome of trauma resolution, the durability of the repaired portion of the reality system, will depend on the thoroughness of the loss resolution method utilized. This is why TRT is designed to be as comprehensive as it can be.
Summary
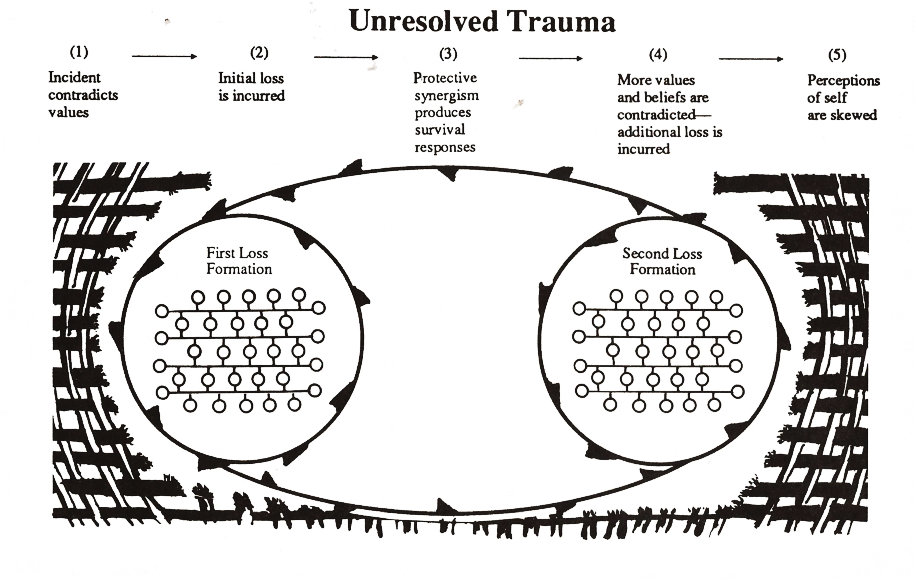
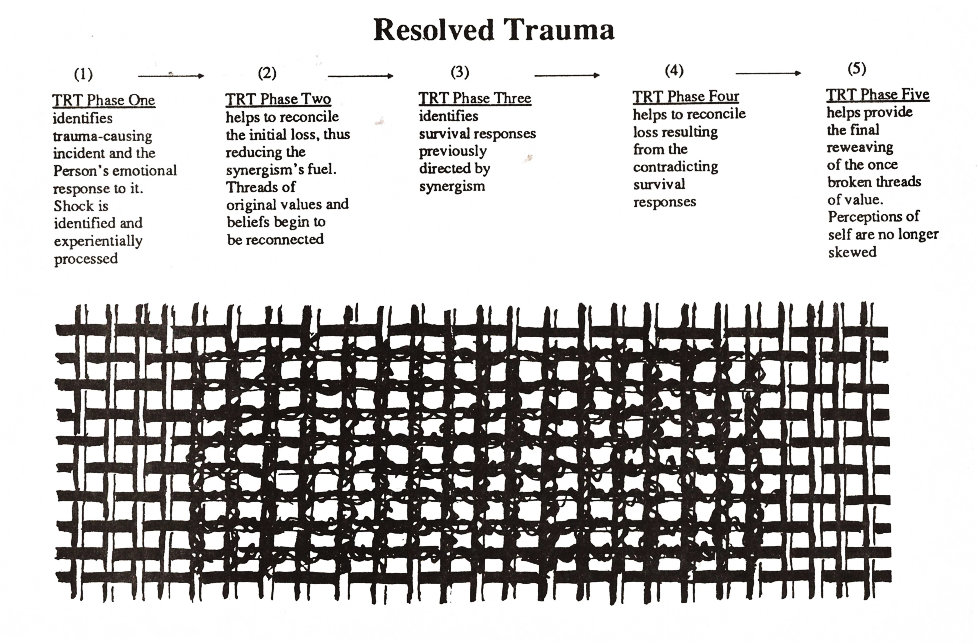
The following graph (Fig. 10) summarizes the loss formation conceptualization of the post-traumatic stress experience and the relationship of the TRT process to that experience’s reconciliation.
Fig. 10 Summary of trauma and trauma resolution processes
Appendix Theory
The theories represented in this booklet were originally developed for the purposes of explaining to professionals how and why TRT works. The concepts of the Mazes and loss formations were derived from our observations of many incidents of trauma being reconciled and resolved. Through these conceptualizations, therapists and counselors learning to facilitate TRT are provided a map and guide for helping others through the trauma resolution process. These conceptualizations are also shared with you in the hopes that they bring clarity of direction and understanding to you, thus making your trauma resolution experience simpler and easier.
- Mental health or crisis management professionals adopt necessarily tough (self-protective) approaches to the process of helping others. However, those individuals' personal values are still effected by the helpers' experiences of the victim's trauma (see the TRT series for Crisis Managers)↵
- Many kinds of compulsive behavior are found to result from brain chemistry and are not necessarily related to trauma.↵
- In addition to the more obvious problems a toxic central nervous system can cause a therapy session, the trauma resolution process can also be adversely affected if sedatives (including alcohol) are used on days other than when TRT is actually conducted. For example, if a TRT session is held on a Wednesday, the therapy will initiate a specific aspect of grief resolution that will continue to be addressed at both conscious and unconscious levels throughout the week. Should the participant drink for social or entertainment purposes on a Friday or Saturday, the central nervous system will be temporarily anesthetized. Even though the anesthetic effects are only temporary, they will still block the otherwise naturally progressing grieving experience started on Wednesday. The net effect of the periodic use is that the survival / protective system of thought will be supported. This support is analogous to the springs of a trampoline that keep the canvas taut so that it always bounces back to its original position. In other words, a TRT participant can work very hard in the TRT session, and then unknowingly reverse his or her achievements through the temporary sedations.↵